

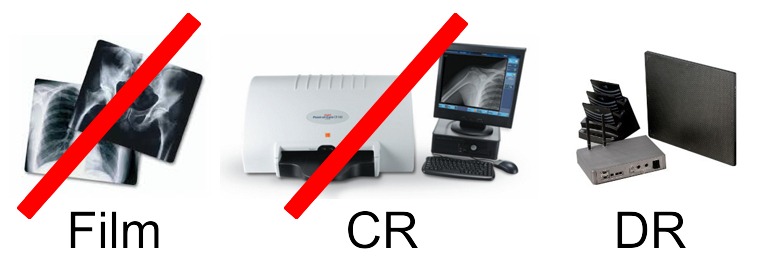
Ever since we learned that the Consolidated Appropriations Act of 2016 would reduce reimbursement rates starting next year, people have been asking why this change? Most people understand the 20% reduction for film studies…it’s another strong encouragement for all medical history to be available via electronic media, but why is the government cutting payment for CR studies eventually by 10%? Why the decimation of CR over DR?
I haven’t gotten a good answer. The only answer I’ve seen is to encourage adoption of the latest technology.
However, I don’t see that this reasoning applies to CR. There is both an economic and patient care argument against this.
Once you have read this post, please let me know if I’ve missed anything and I’ll pass your comments on to others. There are a lot of us who don’t understand.
The Economic or “Workflow” Argument: The move to DR will significantly improve workflow.
Generally this boils down to the time it takes to process an image. Let’s, for argument’s sake, say that both DR and CR have the same data input requirements and patient set-up time. Since the modality worklist feature can be added to both digital technologies, data input is still the same for CR and DR with or without MWL. What the workflow argument amounts to is processing time. So let’s be generous and say DR is 10 seconds and CR is 90 seconds. If you assume that in an 8 hour shift one will work a maximum of 7 ½ hours, then a facility would have process to 338 images a day to save one full time employee. Numbers of this size are found in only the very busiest imaging centers or hospitals.
These numbers assume that the tech is working full out doing nothing but processing images. But there is a lot more involved in taking images, including machine setting, patient positioning, setting the collimator, etc. When one CR plate is processing, the tech is doing other work and when using DR the tech still has to do some or all of these functions between images. This means that our assumption of an 80 second advantage for DR is just not realistic. The 338 images/day number is most likely much higher.
Only institutions that do hundreds of images a day can make a solid justification that workflow justifies DR. One has to find the extra money somewhere to pay for DR over CR and the workflow argument does not seem to be a slam dunk. If anyone has seen a study proving reductions of FTE’s using DR vs. CR, please share it.
The Patient Care Argument: DR technology is superior to CR technology when considering patient care issues.
 Here I’ll take a back seat to a professional who I respect. Meet Dr. Ian Mclean, DC, DACR, and Director of Radiology for the three campuses of Palmer Chiropractic College. He manages three clinics, an outside reading service and the teaching of radiology to hundreds of students each year. He was an early adopter of digital technology, having the schools purchase then best of breed equipment including CR’s and DR panels. He has seen images from a wide variety of CR and DR manufacturers.
Here I’ll take a back seat to a professional who I respect. Meet Dr. Ian Mclean, DC, DACR, and Director of Radiology for the three campuses of Palmer Chiropractic College. He manages three clinics, an outside reading service and the teaching of radiology to hundreds of students each year. He was an early adopter of digital technology, having the schools purchase then best of breed equipment including CR’s and DR panels. He has seen images from a wide variety of CR and DR manufacturers.
Here’s his statement: “The issue not discussed is the wide variation in imaging quality with DR systems both in terms of patient dose and image quality. DR includes not only traditional TFT panels but also CCD based technology, which is not equivalent. Direct flat panel detectors generally provide excellent image quality and are the preferred device for most radiology departments that can absorb the relatively higher cost. While CCD panels have a relatively low cost, the necessary dose tends to be higher and image quality is not optimal.”
“There are also a large number of CR units available that also provide excellent quality images at a lower dose than many DR panels. The discussion should be focused around quality and dose benchmarks rather than one digital technology over another.”
Underlying Dr. Mclean’s statement is the point that the government’s reimbursement decision could have the unintended consequence of hindering technology development. What’s to say that CR workflows can’t be improved or another technology can’t challenge DR?
Another point that I’ve discussed with Dr. Mclean and others is that this reimbursement decision may limit access to imaging. In effect, this decision forces providers to move away from CR and adopt a more expensive technology. For those who have recently purchased CR, it forces on them a new and harsher financial justification for this CR decision. It is very easy to see that practices could simply walk away from their imaging departments, forcing patients to go to more remote, larger centers and less immediate care.
So why was this reimbursement change made? Do you know? If so, please share.
Was it simply “new is better”? Was it workflow (miscalculation)? Was it one manufacturing group making a larger impression on regulators than another? Or was it just a mistake that should be corrected?
I think most of us agree that moving to a full digital imaging environment is best in the long run. We “old guys” may think fondly about the “film days”. We will laugh when our grandchildren cannot tell us what “x-ray film” is just as we have chuckled when our kids asked what an “LP” is. But some changes are good and I think most of us believe that, all things considered, digital imaging is better.
However, if the goal is to move practices to “digital,” then CR should remain an equal to DR. It is more affordable than DR, especially when one considers the large number of quality used systems that are coming on the market as larger providers move to DR, These systems could be purchased by small practices that are still film-based or using CCD DR or earlier generation CR.
Let’s go digital, but let’s do it in a way that is affordable, that encourages maximum quality and minimal dose, and that provides a level playing field for all manufacturers and equipment providers.
What do you think? Please let me know.
Daniel Giesberg – giesberg@amdtechnologies.com – 1.310.471.8900 ext 300




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
I believe it is strictly an attempt to reduce radiation. Although Dr Mclean (according ti the article) states CR dose rates are less than DR in some cases – I am not aware of any CR system’s where this exists. My understanding is film even requires less dose than CR. The order of least to worst dose is DR/Cesium, DR/Gadox, Film, CR. Although I am not an expert, most tables I have seen subscribe to this theory. I am not sure why there isn’t a bigger concern with CT scans where radiation is much greater.
I agree with Dr. Mclean. Sooooooooo what can we do to educate the uninformed legislatures who made this decision?
Good article Dan, I believe the statement referencing specific manufacturing groups is correct. I would expect this decision to be challenged as the process of reducing the reimbursements moves forward. Long Bone and Scoliosis studies would be a good examples of CR being preferred by some.
It’s called churning.
Gregory H.
Hi Dan, I like your posts!! In answer to the reimbursement issue.. DR is less patient dose, even from CR. I hope this helps!!
Have a great day!!
Bonnie B.
Dan: Did you read the links that were published on this on Aunt Minnie?
.http://www.auntminnie.com/index.aspx?sec=sup&sub=xra&pag=dis&ItemID=113334
Medicare Reimbursement Cuts to X-ray by Technology
X-ray Technology Year Implemented Reimbursement Reduction
Analog 2017 20%
Computed Radiography 2018 7%
Computed Radiography 2023 10%
Digital Radiography None None
https://www.advisory.com/research/imaging-performance-partnership/the-reading-room/2016/02/x-ray-reimbursement-cuts
You will notice that this was planned for purposes of law a few years ago. That the process was assisted by Varian Corp is noted. Crony Capitalism. Varian who makes DR detectors saw an opportunity to influence the situation and took it. Granted, it is not Varian specific,
but a boost to one market segment (DR) opens their doors to sell more detectors, maybe even cheap ones made offshore but sold under Varian’s label, or to Varian’s benefit.
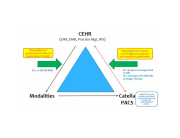
The theories they used have long been used by us marketers to sell DR, but we first considered cost on which choice to offer and stress…primarily, we tried to sell the one, CR or DR, that best suited the end users practice and budget. The arguments of throughput and dose that Varian gives are classic ones, and are aimed at the hospital market. The goal of centralized healthcare is to drive patient care towards hospital (the most expensive, historically, of providers). It is why hospitals have bought up groups and employed “Hospitalists”, and are busy building a “hub and spoke” system of feeding patients from urgent care type facilities all the way to the hospital.
X-ray dealers benefit from this in many ways, but also lose opportunities.
But, the overarching question is does it benefit patients, and what are the costs vs care provided?
Ted H.
Dan
It would make sense if you know the dose needed for good CR images is more the the standard dose needed for X-Ray film.
Film is at 400 speed and The typical CR is 300 speed on average. So although the Digital image benefits of CR and DR are the same, the dose needed may be a factor.
DR dose have dose differences as well depending on the manufacturer, software and most importantly the scintillator used. Cesium being the best for low dosage. And equating to 600 and greater speed. Gadolinium oxisulfide, ( Godox) is typically 400 speed.
I hope that provides some insight.
John S.
Thanks for the comment.
It is my understanding that “DR” units using CCD technology are more like >200 speed systems and some of the earlier CR have the same issue.
So the issue may be less which technology is the right “digital” technology and more setting a patient cares standard that might include dose considerations.
The other issue is the imputed cost to the patient and health care system. By focusing on dose rather than type of technology CR may trump DR for lower use facilities.
The people, as represented by the government regulations, get better health care via dose considerations and more complete digital records AND cost is keep as low as possible by allowing the most cost effective technology find the proper users.
Dan
Hi Daniel,
There are only two reasons I see why this was put in. The first is the DR plate manufacturers saw an opening to get the government to force people to buy their product. Got their lobbyists working and got the amendment inserted. The second is a government employee writing the law had no idea CR was a digital form of x-ray. Either way it’s our government writing unwanted laws that make things more expensive for the general public without any tangible benefit.
Raymond M.
Dan,
I liked your article on Why digital reimbursement rates make no sense. If I had to weigh in with my gut feeling as to why the government is forcing this ridiculous policy on x-ray providers, I would be very suspicious of GE’s involvement at the lobbyist level. To my knowledge GE no longer manufactures CR and would love nothing more than to push customers to buy DR, which they do sell. Remember the president chose GE for some national policy advisor role or some sort and the next week GE announced they were moving all their US production to China. In other words, GE has a lot of pull in Washington and no regard for who they piss off. I can’t think of any reason the government would impose this stupid policy without some outside influence from a high level facility. What does the government know about digital x-ray, dose rates, image resolution, modality work lists, work flow or anything else in that world? What I can’t believe is that we have heard no blow back from all the CR manufactures out there. I can’t believe they are content to let that segment of their market just die off without a fight. After all as you pointed out, not all providers with CR will convert to DR because of this mandate so if these CR manufactures are hoping to get DR sales, it might be an empty hope on their part.
Keep up the good work.
Thanks, CK